The current coronavirus pandemic has been frenetic and a scary time for all. At Oaktree Connect, we urge you to at stay home as suggested by the government. However, this period of time does not have to be all doom and gloom! For most of us, our day to day lives are very busy and we are always on the go. How many of us have thought ‘I don’t have time’?. If you find no positives in this situation, take this as one of them: you have been given the gift of time. In this post, read on for tips on how to fill your new-found time.
It can be very stressful constantly trying to stay up to date with the news and scrolling through social media. Therefore, it may be wise to take breaks from hearing about the pandemic so try to have a tech-free hour! In current times, we are so immersed by technology. Challenge yourself to try something new for an hour.
Exercise is really important whilst we are trying to practice social distancing. Research shows that exercise has benefits for physical well-being as well as mental health. Exercise has been proven to help with decreasing symptoms of depression and anxiety through the release of endorphins.
If you love learning and want to feel productive, stimulate your brain by taking an online course. There are many free online courses in a variety of subjects with just a google search, there is no doubt that something will spark your interest.
Cook something new! Personally, this is something that I have been doing. I am not a great cook, but I have found cooking to be very therapeutic and it has helped me to feel productive. I recently and successfully made pizza from scratch and this has inspired me to explore more recipes. Let us know below if you have recently tried a new recipe!
Have you been meaning to unwind but until now you haven’t been able to? This is the perfect time to have a movie marathon. Let us know your favourite movies below.
Stay in touch with loved ones. Is there a friend who you haven’t spoken to in a while? Why not call, text or video call them? This is a perfect time to reconnect or strengthen social bonds with those who are dearest to us.
Structure your day. Time can seem never ending as there is so much of it at the moment. It can be good for your mental health if you like to have structure and stability. Chunk your time into work and social time to make sure your day is well rounded.
Self-isolation, although tough it doesn’t have to be boring and unproductive. If the above activities are something you have been doing recently, let us know in the comments as we would love to hear from you. Alternatively, if you have further suggestions, we would also love to hear from you too! For now, stay safe. Stay strong.
Through persistent denial of the looming, black “ bellied thunderhead of his shadow, she had tried to keep still “ as still and as quiet as a bunny in a bush – for one move, one rustle, one hitched breath and he’d see her. She didn’t want to look at him. She knew she shouldn’t through years of learning that one look was enough. Calypso Barbie when they first met.
“Hello, Penelope, my name is depression did Santa bring you lots of nice things today?”
A blood stain on her summer dress, the sixth form exit button, Lady Macbeth, gin. And now, famished through the weight gain, through the medication, through the doctors and a cauliflower for dinner.
“Why, Penelope, you know we really shouldn t keep meeting like this.”
She stared down at that pathetic cauliflower before her and felt her foot slip, the brambles in the bush snapped and seemed to cackle, she caught her wrist on a thorn and everything that she had been hiding from billowed in the air and fell upon her like a 50-mile-wide, black parachute.
“What’s the matter? Are you not enjoying your cauliflower?”
Through time and familiar sights and smells one can sometimes run but where is there to go when the innocuous cauliflower is no longer just a cauliflower and produce turns trigger.
“No, I’m not.”
“Well now,” he said. She felt a familiar hand rest lightly upon her shoulder as he bent down and whispered in her ear with that intoxicating purr she both missed and loathed.
“What a pity.”
Dear mum,
Please forgive me, please don’t blame yourself, I know you may not understand, and this is selfish.
In placing a heavy chess board between herself and her mother, chequered with life and death (was her mother white or black? Is death white or is death black?). He once again accompanied her to therapy and split a gut at the comedy.
“TRIGGERS,” he bellowed, clutching his stomach, “Why this fellow should do stand up.”
He went with her on long walks.
“Gosh, isn’t nature ugly. Look at that fat ox over there, trying to better himself.”
He sat with her when she tried to read.
“I wrote this book, you know,” he said, leaning over her shoulder, “Silvia Plath, pure plagiarist.”
He kicked things about her room when she tried to tidy, he sprinkled soiled cat litter on her food, he tucked her in at night and kissed her forehead, he stroked her hair in the mornings. She lay with him, lovingly cradled in the crook of his arm. He listened to her, he smoked cigars and watched her from across the room. “You will always be someone to me, Penelope.”
Dear mum,
I don’t want to ruin your life and hate that you might not now ever have a merry Christmas or that you’ll forever live in dread of my birthday, a day in remembrance of a life given and then thrown away. But I hope that you will come to see, in time, that all the other days are actually all the better. You’re a great mum.
Picked up by the nerve strings, the pickup – or rather the drag down – is merely preliminary and he rarely bothers with it himself. In his tricky subterfuge, he recruits his cabinet to break her so he can play the hero.
First, there comes the woman, with her taunting beauty and her words spoken so sweetly – a vacuum in and of themselves – with a sinister distractedness, she prods at the flaws on Penelope’s face.
“Did Satan spit you out? You’re just so ugly.”
The ever-self-destructive profligate, stinking of vodka and poking Penelope with a gnawed toothbrush.
“You’re hungry. Here, you can take it out again afterwards.”
The fearless musketeer and his watchful python.
“What’s the matter, Penelope? Why I think you’re having a heart attack, you’re choking, you can’t breathe.”
The hag of the haunted house.
“Do you remember, do you remember, do you remember?”
The petulant child.
“That therapist is a hateful brute!”
And the old man and his wild and frenzied raven, who give her sticky thoughts – thoughts that stick to everything, so that she can blindly appreciate nothing. They make her teeter and question, gulp sulphuric pus in wondering – am I? Should I? Will I? Did they? Is that true? With each one of them a kettle weight, the descent is perpetuated by a heavy thought process, until he catches her like a dark prince and the mind begins to melt as if doused in acid, seeping through the eyes. “I’m not crying, my mind is melting” into a world of HE.
HE is the solitude of a dripping tap, the mould eating the plaster, the cockroaches, the infestation. HE is the old man weeping in a broken chair, his mind melting. HE is the girl who opens her legs and immediately feels the need to apologise, her mind melting. HE is the waste that chokes the seahorse and dirties the plumage of the noble swan, HE is the bullet that fells the proud stag, the warm needle in the shivering vein. It is HE, who suckles the breast of every man, girl and abandoned child as the mosquito does blood, who has made her face no longer a face – her eyes do not tear, her eyes her mother will no longer meet, her eyes now the red of picked-at sores. Each organ slows to its final pulsing beat – from tissue to turning leaf and she will soon to be dust.
Dear mum,
I’m frightened, I’m frightened of it and I’m frightened of the battle, the same battle I must keep fighting as his numbers grow while mine diminish. Will I ever be able to turn my back? It is said that Abraham Lincoln used to storm through the woods with a shotgun in his hand on every successive assault.
Two weeks have now passed, and he comes to show her what her life is. She sees herself lying on the bed asleep, or awake dreaming, lying amongst his allies who will never leave her to ensure that she will never leave him. She sees the old hag tormenting the mouse that was her rationality. She sees the fluttering fawn, once her feather of happiness, chained to her self-destruction and covered in cigarette burns. Her beautiful insecurity blows a kiss at the squawking raven as the beloved pet of her fear is snaked around the chandelier and watches her sleep with eyes meaner than cat piss. Linen in anarchy and waste scattered like blasted brick, are swathed beneath the hovering wraiths of her dreams. Above, they twirl and float as the ballerina floats – but their skin has now taken the form of their bones and the residual, oscillating ribbons of putrid hope left to rot, smell of sewage and nicotine.
He scoffed in the face of dreams.
“Dreams,” he’d say, “Dreams are like lily pads for the croaking toad. But one must plop back into the pond to sustain oneself and SNAP comes the cunning water snake. It is better to learn to hide than to fool oneself and forget what is lurking.”
So she let them die. Dreams die a slow death, and they let one know it for the lingering stench.
Dear mum,
I do not feel like a person because I am so afraid of people. Does a zebra fear the zebra as it does a lion? Why is it that when I look at a person s face, they seem less human to me? Why is it that a woman is ugly when she whispers but a man is oh so beautiful? Men do not whisper to me I left the reading and the man thanked me for coming. If he hadn’t thanked me for coming, I’d have said he hates me. But he did thank me for coming and so I say, he hates me. I was in a lift with a boy, when we got to his floor, he walked out too fast. Do you understand, mum? Does this help a little?
“So,” he says. He stands behind her with his hand on her shoulder. The slick black of his cane slices through the periphery of her vison. “How are we doing on the food front?”
“Good. I’m on two weeks.”
“Not a morsel?”
“No, nothing.”
“And your mum?”
“Great, said I look thinner every day.”
“Good,” his voice is warm with stoic pride as he gives her shoulder a gentle squeeze. “You’ve done very well. If you’re sure this is how you want to go about things. There are easier ways.”
“I know,” she answers and swallows down the modicum of doubt once again blossoming, as persistent as the dandelion, in her throat and chest and stomach. “But I’m a coward and I don’t want to hurt anyone. I don’t want her to find me, and I can’t get the note right. It’s better this way.”
“Very well, let’s be off then.”
The gym is empty, there’s no one there, no merciless humming of machines, no jousted joints. He leans languidly against the treadmill and adjusts the speed every two minutes, until she’s on 6mph and can feel her feet and trainers infuse into one static mass. It crawls upwards, ankles now frighteningly numb, then the knees begin to lose pressure.
“I hate it here,” he scoffs. Disgust etched on his face with a hard grimace, he observes the room from beneath the velvet rim of his top hat as if afraid to expose his eyes to the pungency. The place REEKS of endorphins.
Endorphins are good for people.
“Endorphins are a lie!” He snaps and fixes her with a hard, penetrating stare that seems to manifest as a ringworm in her gut. “You feeling anything yet? Chest pains?”
“I feel sick.”
“Right stop!” He slams his hand down on the stop button and yanks her backwards by her elbow. His grasp is hard and violent, and yet his face remains impassive as he drags her weak and stumbling to the door.
“Why did you stop me?”
Because, turning to face her and cocking his head in mock perplexity which makes her shiver. “You’re going to faint, and a fainting spell will only work against us. On to the next.”
He takes her to the city centre, his cane tap tap taps against the cobbles – it sounds like the beating of a rusty heart. They sit by the fountain and the ice-cold marble travels up her spine, from arse to aorta.
“You’ll get piles,” her aunty Beth used to say. The bottom of the sleeping fountain is peppered with coins, clutching the dedicate little wishes of children. In the daytime they glimmer and twinkle like rebellious stars, but in the dark they lie in the murky water dead and dirty and useless. There are no stars in the sky tonight. Drunks stumble about beneath, laughing coarsely like syphilis-infested libertines.
“Well now,” he says, “If your heart won’t do the dirty work, perhaps someone else’s will. Now, make yourself look vulnerable.” He straightens her back and overbearingly lifts her chin with his fingers.
“In case you haven’t noticed, I am vulnerable.”
“No, you’re too hard in the face.” Leaning in close, he winks with the dark luminosity of an onyx and murmurs behind a wayward grin: “Sweet little girls are much more fun to strangle.”
Dear mum,
I know I shouldn t do this, I don’t want to hurt you. I tried, I promise I really tried but I can see nothing and feel everything while empty and the still silence thunders and I can’t catch my breath while I sleep. The man sits there, before the girl without a gun to her head so he’ll just talk to fill the time. There is wanting to die and then there is dying, is there? The man sits there, before a withering mess who wants to die but is not dead and is therefore, as he declares, contradicting herself. Then he leans back in his chair oh so pleased with himself for isn’t he clever? Check mate. I am contradicting myself? Of course, I’m contradicting myself! By definition, the suicidal mind is a contradictory mind. A mind that has found a way to deny the very nature of its being, the most primitive and potent instinct engrained into us since the beginning of man, self-preservation, survival. So yes, well done, alert Sweden, I AM contradicting myself. I am choking on my contradictions. For example, do you know how frightening it is to feel nothing?
So, she tries to smile and cross her legs like some languorous starlet or the silk-clad concubine. She tries translucence, amiability, panting puppy, sex kitten, lucid and gagging for it, pissed and pleasantly puzzled, but, despite her best efforts, she remains unnoticed. In an indolent oblivion they move past and around her as merely blurred outlines and they can no more see her than she can see them.
“Unfortunately,” he declares, to her relief, “I don t think you are going to get anything out of this lot. Nothing but horny little boys, Eros without an aim for his arrow and abandoned old dogs! Not a psycho in sight, the bold-eyed slatterns. Don’t worry,” he adds, slipping his hand into hers, their fingers entwine like slithering smoke, “You will always be beautiful to me, Penelope.”
They arrive back at Penelope’s house and walk up the back stairs.
“Penelope,” he says suddenly, breaking the silence. His voice is quiet and serious, equal parts assertion and interest. “How do you feel about South Africa?”
“Why?” She answers. She is devastated and baffled to need to use the bathroom, why is her body still working? She looks down at her shoes, they shrivel with every step to the tiny toes of a toddler. “These shoes don’t know where they are going,” she thinks.
“Well, you know sharks have an excellent success rate. SLOBS!” They find Penelope’s room still and quiet, permeated only by the occasional, tepid murmurings of a room asleep. Even the Raven, usually blabbering on with the hardy vigilance of a tomcat, was snoozing upon the old man s shoulder.
“Slobs,” Depression reiterates through gritted teeth, “Don’t I do enough! Oh, Penelope, why so glum? We can try again tomorrow.”
“How about you just go away,” she answers. She sits down on the edge of her bed. Her eyes, limp and painfully hooded, are blunted with the inertia of being open.
“Why would you want that? I mean, look at all these wonderful books I have allowed you to keep. Have I not been very good to you?” He wanders over to the book shelf and begins picking them out one by one: “wrote this one,” flings it over his shoulder, “oh, and this one too and this one, why, you’ve got some of my best works here. Ahhh, No Longer Human, I must say Dazai was a pleasure to work with.”
“Don’t say that,” she snaps. In that moment he sickens her. His callousness sickens her. His unabashed vulgarity starts to fill her with a formidable revulsion that begins to steam through her body, until, eventually, it groans and starts to clatter and clang against its russet tracks, breaking down somewhere around her left leg.
“Oh, and why ever not?”
“Because he killed himself.”
“I know,” he says, half turning, still with Dazai s book in his hand, and throwing her that salacious wink she could neither resist nor bare to look at.
“Well, it’s in very poor taste, even for you.”
“Poor taste? What other option was there? Of course, there’s always therapy,” he retches and spits the word out as if coughing up phlegm. “But does the artist live longer through the latter?”
“It depends on how you look at it.”
“It depends on nothing. Therapy aims to untangle the web, but without its web, how will the spider eat? Intriguing little creature, the spider. Most will see one, scream in revulsion and pounce to a nearby perch. They wait for it to scurry away and yet they can never quite stop staring at it. No web, no spider. Imagine that. Look at him over there, with his slippery snake can you imagine a world without him? A world without fear?”
Dear Mum,
I can’t see anymore. I have two friends, one is a god to me and the other makes me laugh, but I can’t see anymore.
“Can you imagine a world without crippling insecurity, pain and bladesmith memories that sharpen their knives upon the bone?”
Dear Mum,
I love you.
“No planned, well devised, bordering meticulous schemes to destroy oneself?”
Dear Mum,
I hate you.
“No questions, no answers, rose petals in the place of blood?”
DearMum,
I’m sorry
“A world without ME?”
Dear Mum,
I love you.
“Do you think it would be a better place?”
“So we should all just be miserable. For the sake of the so-called spider?”
He approaches and crouches down before her – his long fingers entwine around the tip of his cane as his dark eyes gleam within the hollow shadows of his face.
“It depends on how you look at it,” he answers. There’s an undertone of mocking in the forlorn resonance of his words, in his voice coated in silk and sugar. With the tranquil stillness of a lily pond, he smiles the lazy, slow smile of a prince, of the insatiable wolf, of the devil courting.
They sit in silence for a while. She keeps her head down, he bores into her. She is thick, she is sloppy, she is a viscous blob of distilled meaning.
“You want me to die,” she whispers. She feels her throat tighten and close over the word die – that serrated, final word that can mean one of a million different things while thought, definition and meaning flap about inside her skull like bats with broken wings.
“Do I? I don’t recall telling you to die. I recall you wanting to die and, as always, I have offered my unflinching support. But, don t confuse things, Penelope. Death at the hands of oneself is the purest choice a person can make and, contrary to consensus, is totally detached from one’s afflictions. I am what you make of me.”
“I hate you.”
“No, you don’t,” he calmly asserts. “I only want what is best for you. I want you to be who you are.” He shoots his hand out and pinches her chin between his fingers. Locked in a struggle of submission and fear and a cloying need, their hard indent forces her eyes up to meet his. “And I am a part of who you are.”
Her self-destruction, draped across a chair and holding an empty bottle close to her chest as if it contains a love letter from captain Morgan himself, snores a resonating grumble from the depths of her gullet. Depression sneers over at her with searing contempt and with one giant swoop of his cane, bonks her on the head shouting: “GET UP! We’re leaving.” Suddenly the room leaps awake with feigned alacrity as the insidious glitter in the eyes of his flock is replaced by an embarrassed submission that never fails to surprise Penelope, the fire breathing dragons now doe-eyed and wheezy.
“Are you going?” she asks.
“Must, I’m afraid, got a meeting with a chap in Canary Warf. You know, there’s nothing like the newly bankrupt to keep me feeling young.”
“But I’ll be back tomorrow,” he coos and smiles down at her. It’s a warm smile, a tender smile, but a smile written in cypher that speaks of the interspersing paradox hidden beneath. “You will always be special to me, Penelope.”
After he leaves, she sits listening for the tender tweeting of a wagtail outside her window, the one she sees every morning. It probably isn’t the same one every morning, but she likes to believe it is – and has named it James Brown for its funny little wiggle. But delicate little birds are not accustomed to singing in the dark and are often replaced by the lonesome cawing of a distant fox. Delicate little birds that can shit on the head of an unsuspecting child, replaced by the ruthless fox, howling like a banshee, that was also the charming and irreverent Basil Brush from her childhood and teacher to the lost little prince.
Dear Mum,
I suppose things are not always what they seem and the things we see are like clouds in the sky, lured by shifting currents of air. The trees are bare. They have given the last of their bounty to the earth and remind me of emaciated orphans, naked and waiting. I can’t see the clouds, but I know they are there for the sky is black – thick and heavy, its velvet veil seems so impenetrable even the wind can’t billow its weight. I don’t think I’ll ever see through that sky. But then, as I sit in quiet submission to the vast desolation above and the good in me labours to breathe, suddenly the sky reveals an imperfection. Blown by a distant wind like the metamorphosing wind that pursues the caterpillar – that thick, imposing curtain becomes merely a gossamer wisp of smoke, unfurling before a lone star- or is it Venus? Was it always there? I’m not sure, it doesn’t matter I suppose, it’s there regardless. Perhaps if I hadn’t looked closely at the sky just now, I wouldn’t have noticed it at all- a hopeful wink amidst the waves of shifting darkness, there incomparable merely waiting for a wind to shine its shoes.
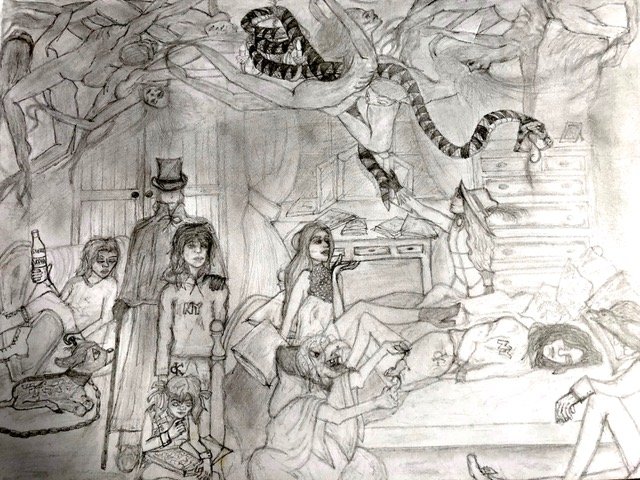
A Patient has been having treatment with us at Oaktree and written an account of her experience. She would like to be a published writer and has agreed to share her story with us. The sketch is also by the Patient. [Note: Patient’s name has been edited due to privacy]
It’s one of the most common questions we get asked. Of course, patients want to know what will happen before, during and after a TMS treatment.
Our experienced and caring practitioners will guide you through the whole process and be by your side every step of the way, but here is a quick guide on what to expect.
A Full Assessment with Oaktree
When a patient first calls, we offer advice on what TMS can achieve as a treatment, guidance on costs and the usual length of a course of treatment. If the patient would like more information and advice, one of our consultants will then arrange a free call with them to discuss if TMS will be an effective form of treatment for them and, if so, how TMS could work for them.
If they would like to go ahead, we invite them in for a face-to-face mental health assessment and the chance to see the TMS equipment for themselves. The consultant psychiatrist will assess the current and past issues and background to come to a diagnosis. If TMS is considered an appropriate treatment for them then they will talk through everything that happens during treatment, including the sounds and procedures, so that they know exactly what to expect. From there, we create a bespoke care plan and discuss the treatment options with them.
As TMS does not affect you physically, no physical assessment or investments are needed and, once the patient has signed the consent form and is happy to go ahead with TMS as their preferred choice, the treatment can begin immediately.
We invite patients into the therapy room, where they can relax in the treatment chair. It is similar to a dentist’s chair. Patients will be asked to wear a cap over their head and we lightly mark this cap to indicate the area of the brain that requires treatment. We then carefully lower the coil over the patient’s head ready to start. The coil looks like a large figure-of-eight plastic paddle and it very lightly touches the scalp. We use Magstim TMS systems, the pioneers of the technology.
The patient will hear a series of loud clicking noises and a light tapping on their head under the coil but it is completely non-invasive and pain-free.
During treatment patients need to remain still but they can listen to music, watch a TV show, or have a chat with the clinician. It is completely up to them how they’d like to spend that time. Many use the time to catch up on some rest.
Once the treatment is finished, which varies from a few minutes to half an hour depending on their care plan, they are free to go about their day as normal including driving or returning to work.
Incredible results
TMS is a very simple treatment that can achieve incredible results. Treatment times vary from patient to patient but we often see results in just three weeks of daily TMS sessions.
TMS can be easily be incorporated into a patient’s day with very little disruption and – most importantly – it really works.
Schizophrenia is not the most understood of mental disorders. Oftentimes it is confused with Split Personality Disorder, when in reality it’s less cinematic and a lot more traumatic. Below is a poem inspired by the condition written by our psychology trainee, Anjili Gogna.
The sounds of voices, the unpredictable noises Leaving me confused but people tell me there’s no excuse The deterioration of my health Has encouraged me to find help
Nobody understands what it is Questions rise like tides in me too A never-ending cycle of pain and despair I wonder, does anyone care?
The thoughts that trouble me, is that man here to kill me, Or complete apathy, to the world and creation, This scares me and adds to my frustration, I turn to highs and drink to forget about my life on the brink
Some call it a mental disorder, some are plain harsher Everyone seems against me, ridiculing me or worse pitying me Leaving me very lonely and sad and completely mad Is this the madness everyone talks about only that?
Recently, I came across some help, Finally, someone could offer more than just resent, For once they called me a person with schizophrenia, Offered me medicine, talked with me rather than show hysteria, This helped manage my thoughts and the annoying voices just disappeared.
Now the day has arrived that I will make a brave entrance, Into this world that is new to me, I feel safe, it feels right The sight is clearer, possibilities are brighter There’s a sense of relief, gone is the despair Now behold, at last I am on the repair
We all know what stress is, but it can be hard to put into words. For one, there is no agreed definition. Stress is an overwhelming feeling in response to a situation or events that put us under pressure. Stress is also the effects on our bodies of these pressures.
In a recent poll by the Mental Health Foundation, three out of four felt so overwhelmed by stress that we were unable to cope in the last 12 months. Overeating and eating unhealthy food were the top coping strategies and were used by almost half of the respondents. One in three used alcohol to cope, and one in eight started or increased smoking.
All stress, however, is not the same. There is good stress, which motivates us to do our best at the things that matter. Small doses of good stress, for example in preparation for an exam, can help in keeping our focus and enthusiasm towards whatever we are trying to achieve. But beyond a healthy amount of stress, both health and performance deteriorate. Here is a two-step strategy to keep stress under control.
Step 1: Recognise when stress stops being helpful
Learn your early warning signs. These are the first signs that you might be experiencing more than just good stress. Examples include:
Physical exhaustion
Forgetfulness
Difficulty concentrating
Procrastination
Restless sleep
Avoidance of people or situations
Overeating or loss of appetite
Relying on junk food and alcohol
Not feeling your normal self
Feeling ineffective
Physical symptoms without a physical cause
Irritability and tearfulness
Difficulty relaxing
Low self-esteem
Step 2: Improve your coping skills
Prevention is better than cure. Once you notice the first signs of stress, take action:
Identify the underlying causes
Focus on what matters the most
Take a step back and look at the bigger picture
Talk to supportive friends and family
Eat healthily, reduce smoking, alcohol, and caffeine
‘People often assume that Connor must be amazing with art or music. He’s very bright but in a very unique way. He struggles to understand the world the way we can, but sees and senses so many things that other people don’t.’ Father of Connor, 9 years old with autism
In this current day and age, autism awareness is growing exponentially. However, there are still many common misconceptions about autism held by many, which can cause issues with autism being recognised and hinders support being provided to the people who do suffer from autism in a variety of ways.
Here, we want to shed some light on these misconceptions and most commonly held myths with the hope to be able to change thinking and attitudes towards this neurodevelopmental disorder.
Myth 1: AUTISM IS LINKED TO VACCINES
Possibly the biggest and most damaging misconception is the claim proposed by Andrew Wakefield, that the Measles, Mumps and Rubella (MMR) vaccine causes autism. This fraudulent claim led to the public disgracing of Dr Wakefield for a number of reasons and his claim was repeatedly disproven in subsequent years in many high quality research studies that proved there was no link between vaccinations and autism.
Myth 2: AUTISM IS A DISEASE
Contrary to popular belief, autism is not a disease. It is a developmental disorder characterized by differences in communication, behavior, and social interaction. Viewing autism as a disease implies that it needs to be cured, which can be harmful and misleading. Instead, it’s important to recognize and respect the unique perspectives and strengths of autistic individuals.
Myth 3: PEOPLE WITH AUTISM LACK EMPATHY
A prevalent myth is that people with autism lack empathy, which is simply untrue. While individuals with autism may process emotions differently, many are deeply empathetic. They may express their empathy in ways that are not immediately recognizable to others, but that does not diminish their capacity for understanding and sharing the feelings of others.
Myth 4: AUTISM IS A CHILDHOOD CONDITION
Autism, a lifelong developmental condition, affects individuals in unique ways. While many people commonly associate autism with children, it’s important to recognise that there are actually more adults than children living with autism, particularly in the UK. This highlights the necessity for ongoing support and understanding throughout a person’s life.
Research indicates that with the right support, individuals with autism can experience significant improvements in various areas of their lives. This support can include specialized educational programs, therapeutic interventions, and community resources tailored to the needs of autistic individuals.
One of the areas where individuals with autism can see positive change is in language and communication skills. With appropriate interventions, such as speech therapy and communication devices, many people with autism can enhance their ability to express themselves and understand others. This improvement can lead to better social interactions and a higher quality of life.
Anxiety is a common challenge for many individuals with autism. However, research suggests that with the right strategies and support, anxiety can be effectively managed. Techniques such as cognitive-behavioral therapy, mindfulness practices, and sensory integration therapy have been shown to help calm anxiety and improve overall well-being.
While autism is indeed a lifelong condition, the potential for positive outcomes exists at every stage of life with the right support.
Supporting individuals with autism is a community effort, and by fostering an inclusive environment, we can help create opportunities for everyone to thrive.
Myth 5: AUTISTIC PEOPLE HAVE SPECIAL TALENTS
Many parents of individuals with autism and those with autism are asked this extremely frustrating question and often come across as condescending. It’s important to remember that having autism does not automatically equate to possessing extraordinary abilities. Just like neurotypical individuals, people with autism have a wide range of strengths and weaknesses. Recognising and celebrating these strengths is essential in promoting a more inclusive and understanding society.
There is some truth in the fact that people with autism can have higher abilities in certain functions.
Research indicates that about 28% of individuals with autism exhibit specific abilities that stand out significantly. These abilities, often referred to as “islets of ability,” can manifest in various forms:
Mathematical Skills: Some individuals with autism have an exceptional ability to solve complex mathematical problems, often with little to no formal training.
Artistic Talent: Many autistic individuals possess extraordinary artistic skills, creating intricate and imaginative works of art.
Memory: Enhanced memory abilities, such as the ability to recall vast amounts of information quickly and accurately, are also common.
Musical Talent: Some may have perfect pitch or the ability to play instruments by ear without sheet music.
Myth 6: AUTISTIC PEOPLE HAVE LEARNING DIFFICULTIES
Many autistic people are very able and independent, with the right support and a suitable environment most will do very well in a variety of area of work and leisure.
One common misconception is that individuals with autism who take longer to process information do not understand it. This is not the case. In fact, the unique cognitive processes of autistic individuals can bring about distinct strengths and advantages.
Some autistic people may require additional time to process information, which is a reflection of their unique neurological wiring, not their level of comprehension. This slower processing time allows for thorough analysis and a deep understanding of the information at hand. By taking the time to process in their own way, autistic individuals can often uncover insights that might be overlooked by others.
Strengths of Autistic Individuals
The strengths of autistic individuals can be significant and varied. Among these strengths are:
Attention to Detail: Many autistic people have an exceptional eye for detail, which can be advantageous in fields that require precision and accuracy, such as coding, engineering, and quality control.
Pattern Recognition: A remarkable ability to recognise patterns is another common trait. This skill can be particularly beneficial in data analysis, mathematics, and scientific research, where identifying patterns is crucial.
Focus and Persistence: Autistic individuals often exhibit a strong ability to focus intensely on tasks, allowing them to work on projects for extended periods without losing concentration. This can lead to high-quality work and innovative solutions.
Myth 7: AUTISTIC PEOPLE ARE ANTI-SOCIAL
Autistic people may need extra support with social skills or interact differently with the world around them, but most autistic people enjoy having relationships.
Those with autism express their difficulties in different ways. Some are quiet and shy or avoid social situations, others speak too much and struggle to have normal two-way conversations. Implicit communication can be confusing for autistic people and things such as body language, tone of voice and sarcasm can be difficult for them to read. These challenges can make it difficult to make friends, build relationships or get on at work; things neurotypical individuals often take for granted.
Taking time to get to know autistic people and understand their differences in an environment where they are happy makes all the difference
Myth 8: ONLY BOYS ARE AUTISTIC
Although autism is significantly more prevalent in boys than in girls, it maybe a matter of it not being recognised in girls as much. Girls are more likely to ‘mask’ their autism features, and are more likely to learn the skills to interact with the rest of the world more than the boys. This can mean that girls with autism are diagnosed much later in life than boys.
Myth 9: AUTISM IS CAUSED BY BAD PARENTING
Autism is a developmental disorder and definitely not caused by bad parenting. Research has proved that parenting is not to blame for the causation at all. However, parenting style can certainly equip an autistic child with the tools to better cope with the world and affect their behaviours in the future and throughout life. But it is not the root cause of autistic behaviour.
Conclusion
We need not look at autism as a terrible disorder with a low ceiling of promise, but as a marvelous opportunity to look at the world through a different lens and walk in different shoes. If you or someone close to you needs support for mental health issues, please do not delay seeking out help. There are people who can help you.
Hello all, As we enter the joyous New Year, we look retrospectively at the positive moments that 2017 offered to us. One such moment was the Gatsby Christmas Charity Fundraiser, held here at the Oaktree clinic on the evening of the 1st of December. This was held with the aim of setting up a pro bono fund to subsidise our psychological and psychiatric services for young adults and children who have difficulties fulfilling the financial commitment of receiving care. Here at The Oaktree Clinic, we believe that every person has the right to high quality care, regardless of race, gender and socioeconomic status. Attracting an attendance of approximately 80 people, along with the help of our generous guests, we raised a total of 1200GBP, a massive step towards helping our close-knit community. The efforts of the Oaktree staff resulted in a very successful raffle and auction. The selection of 7 different prizes in the raffle and multiple pieces of elegant artwork proved to be in high demand. Alongside some lovely appetisers, we got the pleasure of listening to two very talented singers: Titine Lavoix and Rhea Deshpande. Drawing all the guests to one room with only their voices, their talents clearly encapsulated the attention of all the guests, singing various numbers from the early 20th century era. Later on, after some more food and drinks, it seemed like the energy of the guests began to bubble over. The power of dance allowed everyone some release. Two instructors from Smooth Salsa Dance Company held an interactive Salsa workshop, a hit with the majority of the guests, by the end, could differentiate their right and left feet! We would like to thank all the guests who attended and all who donated to help make this event a success. Also thanks to Dr Meetu Singh, Dr Minnie Joseph and the Oaktree staff for setting up and carrying out a successful event. Thanks should also go out to the plethora of companies, businesses and the two artists: Alexander Rhys, Patt, John Hill, Mezzo Company, Hair Boutique, and Sky Clinic who donated cash sums, vouchers, and artwork for the benefit of our cause. Artist Biography Pat Short: I design and create highly stylised, organic stoneware pieces. My work is influenced by my passion for the natural world and a desire to create pieces that reflect the beauty of forests, stream and oceans. I trained as a Cartographer and discovered clay later in life when I took some amazing classes at the Midlands Art Centre in Birmingham. http://www.studiopottery.co.uk/profile/Pat/Short Alexander Rhys:Alexander Rhys is based between Birmingham and London, UK. His work has been sold and published in New York, London, Los Angeles ,Chicago and Amsterdam . Alexander Rhys studied Fine Art at Bath Spa University, UK, where he explored the role of Art in Therapy. His unique works manipulate acrylics with the aim to take the viewer on a journey of finding the ordinary, extraordinary. Rhys’ global and diverse clients include outdoor advertising giants Clear Channel and leading Kenyan hip-hop artist Octopizzio Alexander Rhys launched his online gallery and store to provide the opportunity for people to enjoy and purchase his work. Alexander Rhys is proud to be supported by the Prince’s Trust. Alexander Rhys offers a bespoke commissioning service. If you find a piece of work on Instagram or in the Gallery that you would like to inspire a bespoke commission, please email hello@alexanderrhys.com.
Athletes strive to reach their ultimate potential and sometimes even pursue super human targets, attempting to master their own bodies. Testing the boundaries of physical selves, putting themselves through the gauntlet everyday to reach the pinnacle of their individual performance and beyond. The notion of the ‘perfect’ athlete seems to be a chimera in the world of sports for coaches.
An individual fully synergising the multitude of different facets that construe ‘perfection’ is a rarity. Both physical prowess and a superior level of mental strength is needed, but the latter overlooked by many. The willpower, resilience and mental stability of athletes are tested day in and day out, in training and during competitions.
However, the expectation that one can be totally in control of their thoughts and cognitive processes at all times may become unreasonable, even impossible. This effort can then extend to an urge to control the behaviour of others.
The battle between the competing athletes can then begin on two fronts, physical and psychological. One of such ‘psychological warfare’ strategies, which is alarmingly common, to gain a mental edge during competition, is ‘trash talk’. Both players and spectators at all levels of sport use this dubious strategy. Some examples of ‘trash talk’,
“I’m just looking around to see who’s gonna finish second.” Larry Bird (1968-NFL)
“I’m not worried about the Sacramento Queens. Write it down. Take a picture.”- Shaquille O’Neal (2003-NBA)
“Float like a butterfly and sting like a bee…his hands can’t hit what his eyes can’t see.”- Muhammed Ali (Boxer)
Trash talk has been shown to drastically impact on performance, its effect seems to increase exponentially when players are losing as they feel that they have no control over the situation. Their focus shifts from “winning†to attaining a personal victory by satisfying their impulse of retaliation. A lack of respect seems to be a frequent trigger, causing heated exchanges on the pitch and a resultant change in performance.
HOW TO DEAL WITH TRASH TALK
There are a number of strategies one can employ to deal with and prepare for trash talkers.
Mental imagery: visualising yourself in situations where you are resilient and calm.
Self-talk (motivational affirmations e.g. mantras).
Meditation: Clearing your head and maintain peace within yourself.
All elicit positive results, helping individuals tune out negative thoughts (doubts, worries, insecurities) and external stressors (fans and opponents).
Athletes with an understanding of this psychological battle, with well-developed skills in their ability to remain focused will retain composure in the face of trash talk. They fully immerse into their performance, remaining unperturbed by the words of their opponents and WIN.
Author: Varun Deshpande, Psychology Assistant, The Oaktree Clinic
I, along with my colleague, Dr Meetu Singh took the opportunity to attend a conference, with a view to further enhancing our knowledge of the latest research on rTMS (Repetitive Transcranial Magnetic Stimulation). It was a fruitful day! I am therefore taking this opportunity to write about this innovative treatment.
rTMS is one of the new and innovative brain stimulation treatments in addition to Vagus nerve stimulation (VNS), Magnetic Seizure therapy (MST) and Deep brain stimulation(DBS). Electro-convulsive treatment (ECT) is the best studied and utilised physical treatment for depression.
Brain as widely known, is an electrical organ that functions through electrical signals being passed between nerve cells. rTMS uses magnetic stimulation to activate or inhibit this electrical activity depending on the disorder. rTMS is based on Faraday’s law of electromagnetic induction i.e.- electrical activity in the brain tissue is modulated by a strong magnetic field. The rTMS machine produces brief pulses of electrical current inside a coil and this in turn generates this strong magnetic field that passes through the scalp and skull painlessly, activating the neurons in the brain. High frequency rTMS facilitate brain tissue excitability while low-frequency rTMS can suppress activity in the hyper-aroused brain, for example in anxiety disorders. Low or high frequency rTMS can be used solo or in combination, depending on the mental disorder being treated.
Unlike ECT, in which electrical stimulation is more generalized, rTMS is targeted onto a specific site of interest in the brain. Another major difference is that while ECT effects are through causing fits, rTMS causes changes by painless magnetic waves directly stimulating the tissue. It therefore does not require anaesthesia or admission into hospital. Also, this understandably improves the side-effects profile and is better received by the patients. Unwanted effects may include scalp pain, headache or burning sensation locally, none of these tend to last long. Rarely, when given in very high doses (not the currently available and approved doses) it has caused seizures. There is also no loss of memory, unlike that reported with ECT. Patients may complain of scalp pain, headache or burning sensation, which can appear during the treatment and do not last long.
First developed in 1985, it has been studied extensively for use in depression and chronic pain. In 2008, the FDA approved rTMS for use in patients who did not respond to at least one antidepressant medication in the current episode or did not want to take medication due to side effects. National Institute of Clinical Excellence (NICE), UK, approved rTMS for treatment of depression in 2015, after careful consideration of published research. It is now offered in USA, Canada, Germany, Japan, Australia and UK. rTMS has produced encouraging results in treatment of many other disorders both mental (e.g. anxiety disorders, eating disorders, PTSD) and physical (e.g. Post- stroke rehabilitation, tinnitus, migraine, chronic intractable pain) apart from depression.
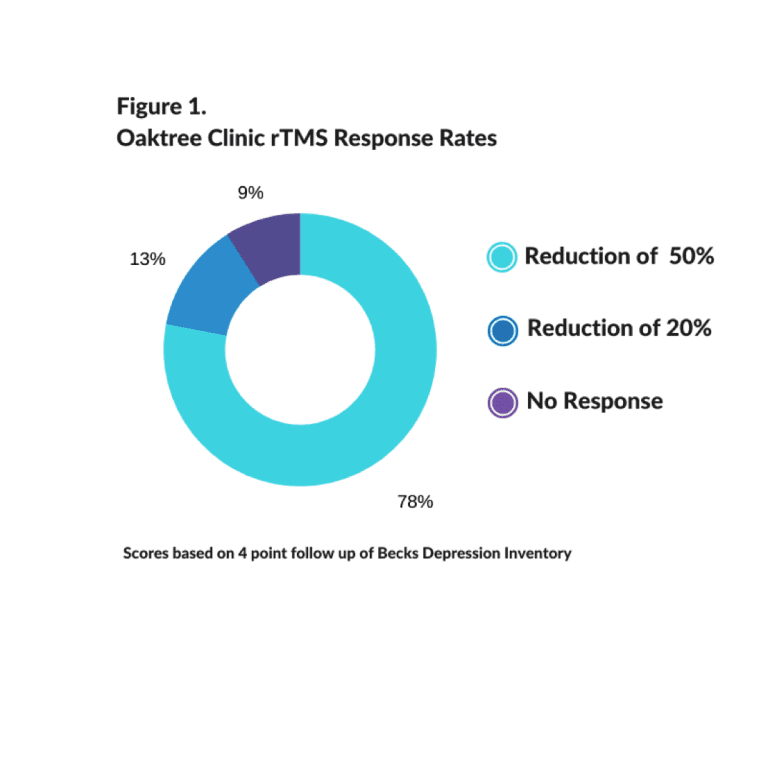
Future of rTMS appears to be bright; as it gradually becomes more known amongst medical professionals as well as patients. Encouraged by the efficacy and tolerance to rTMS, Oaktree Clinic has initiated this service in September 2016. The results here since then with this form of treatment have been nothing short of phenomenal.
Dr Das is a Consultant Psychiatrist with experience in assessing and treating the whole range of mental health & psychological issues in older adults. She works within the NHS and Private sector. Dr Das has special interest in treating memory problems (Adults of all ages), Alcohol & Substance Misuse in Older People and Physical & Mental Health issues in Older People with forensic history.
I recently saw a 72yr old man in my clinic whose family have noticed gradual worsening of memory. He is observed to be missing things in day today life which he previously would have happily paid attention to or remembered. He lives on his own having lost his wife quite suddenly two years ago. He did not cope very well, became depressed, had significant problem with sleep and started to withdraw socially. He was started on antidepressant and hypnotic to help sleep. He had started to take more than prescribed hypnotics, cut down following a consultation with GP. He has started to drink 3-4 pints of beer most nights. He is also on co-codamol for widespread osteo-arthiritis. There is past history of anxiety & depression for which he sought help. He said that he, all his life drank heavily but never had any problem so did not seek help. He has history of hypertension and a lifelong heavy smoker, has cut down to 10 a day recently.
I recently attended a college conference on addiction and in the same week saw a patient (mentioned above) that highlights the complexities an older adult with substance (alcohol/drugs) misuse may face or present to a practitioner. I thought I’d pen few lines down.
The first UK based report of the older Person’s substance misuse came out in June 2011, followed by a comprehensive cross-faculty report on substance misuse in older people in 2015. I am aware that a further review is due this year.
How common is the substance misuse problem in older adults?
The proportion of older adult in the population is increasing and projected to double by 2031. The number of older adults with substance misuse problems is also reported to be increasing. Substance misuse is top ten risk factors for premature death and health problems and rate of death due to substance misuse is more in older adults than younger people.
Substance misuse problems in older adults are most often associated with the misuse of alcohol and over-the-counter (OTC) and prescription drugs. Older adults frequently show complex patterns of substance misuse; alcohol use with prescription medications, tobacco, over-the-counter drugs or illegal drugs. Multiple drug dependence aka polypharmacy is a particular problem in older adults with physical and mental health problems.
In recent data released from Office of National Statistics (ONS) for England shows that Baby Boomers (people aged 45 and over) are drinking frequently and at more hazardous level. Alcohol related hospital admissions have increased by 64% in a decade and highest ever level. A few older adults use illicit substance, mostly marijuana, however this is projected to increase as the over 45yrs old who use illicit drugs, get older.
Majority of older adults with substance misuse problems are simply continuing a pattern of behaviour or addiction that began earlier in their lives and invariably have a family history of alcohol and drug addiction. About a third of older adults develop substance misuse problem in the later years, usually in response to bereavement, social isolation or lack of social support.
Physical and psychological factors associated with substance misuse in older adults
As people age, body loses muscles, gain more fat as a result metabolize substance slowly, develop increased sensitivity and reduced tolerance. The kidneys and liver may not be functioning as well. Alcohol consumption in the presence of other medical conditions or medications may create danger by causing or complicating medical conditions, compound medication interactions and increase falls or confusion. It is not uncommon to find lack of communication between the physician and the older person to allow correct dosing, titration, interactions and side-effects leading to multiple medications being prescribed for medical problems.
Misuse of alcohol and drugs can affect physical health; hypothermia, stroke, heart disease, cancer and poor liver functioning. Psychological problems like self-neglect, anxiety, depression and insomnia are common. Long-term use leads to dementia and cognitive impairment.
We cannot ignore the fact that drinking and drug use can have detrimental effects on the near and dear ones, causing anxiety, stress and sometimes relationship breakdowns.
Difficult to identify the problem
Research show that physical, social, psychological and legal problems associated with substance misuse in older adults mean they are likely to have regular contact with health and social care services. However, early identification of substance misuse is more difficult than in younger people.
The nature and pattern of older adults substance misuse make the problem less obvious; they consume substance at home, in local pubs or in social settings, less likely to be involved in trouble with the police, get into arguments or miss work due to substance use. Research has identified that family, care-giver and clinician may be complicit in the addiction process in the older adults. Substance misuse is a hidden problem and Royal college of Psychiatrists have quite rightly referred older adults with substance misuse problem as ‘our invisible addicts’. Health and social care professional may not always spot heavy drinking or drug misuse in older adults. Older adults may not talk about their misuse due to perception of stigma, shame or embarrassment, the effects of alcohol or drug misuse may mimic physical or mental health problem, and most importantly they are often not asked the question regarding alcohol or drug use as they are assumed not to have the problem.
Pooling help
Health professional generally find easier to treat alcohol and drug problems in older adults than in younger people as they are motivated and want more contact with their family members especially grandchildren.
Older adults who misuse substances may have complex or multiple needs that are often difficult to assess and may warrant further investigations. A comprehensive assessment, including physical and mental health examination is needed. Additional corroborative history, laboratory tests would assist identification.
Screening is a brief process that aims to determine whether an individual has a drug and/or alcohol problem, health-related problems or is showing signs of risk behaviours. Several screening tools are usually accurate in identifying alcohol misuse in older adults; Cut-down,Annoyed,Guilty,Eye-Opener (CAGE); the Short Michigan Alcoholism Screening Test-Geriatric version (SMAST-G); and the Alcohol Use Disorder Identification Test (AUDIT). While screening is important, it may not always lead to effective treatment. Brief interventions e.g. counselling and education at the primary care setting help. Psychosocial interventions, such as CBT, motivational interviewing, as well as supportive, non-confrontational approaches and group therapy for older people are likely to be effective.
Self-help groups e.g. AA exclusively for older adults are better, so do specialized treatments; outpatient, detoxification, inpatient, residential and recovery services tailored to the needs of older people. It is critical to understand, no one-size-fits-all approach.
Limited research to understand medication misuse in older adults show that computer-based and group health education may be useful. Medication leaflets/passports to accompany medications have been helpful. Medication review by professionals at primary and secondary care settings, in nursing homes are recommended. Brief information and intervention sessions represent viable options. Electronic medical records and databases that connect the information systems of physician and pharmacists are effective in addressing the problem.
Support organisations; Addaction, AgeUK and Alcoholics Anonymous all aim to improve later life through information, advise, campaigns, products, training and research.
Dr Das is a Consultant Psychiatrist with experience in assessing and treating the whole range of mental health & psychological issues in older adults. She works within the NHS and Private sector. Dr Das has special interest in treating memory problems (Adults of all ages), Alcohol & Substance Misuse in Older People and Physical & Mental Health issues in Older People with forensic history.
Contact:
Email – contact@oaktreeconnect.co.uk
Telephone – 020 39277699
Manage Consent
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behaviour or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.